
Diseases and borders. Epidemics and disease spread in Scandinavia and the area around the Baltic Sea during the 18th century
Short description
For a long time, it was claimed that crop failure and hunger, in combination with population growth, primarily caused the recurring mortality crises during the 17th and 18th centuries. By the late 20th century the “infections theory”, where social contact and exposure to infections, was rather put forward. However, the problem - highlighted several times in international research - is this theory’s hypothetical character and our lack of understanding about starvation, disease mortality and infections during this time period. In this project, big areas will be excerpted at the level of individual deaths in smallpox, dysentery and fevers in Scandinavia and the area around the Baltic sea. This will allow us to follow the spread and examine it in relation to supply crises, wars and governmental preventative measures to stop the spread.
The most distinctive feature in the demographic history of the 17th and the 18th centuries are the mortality crises. Several times the mortality skyrocketed. For over 200 years, historians and social scientists have discussed what caused these crises. Suggestions have included God’s punishment, lack of food, poor hygiene, war, beggars and overpopulation. Numerous studies have been made with regards to the connection between lack of food and mortality, but the results have often been contradicting mainly due to the infectious. Indeed, there are several horrifying examples of starvation killing people, but at the same time it is clear that it was mainly dysentery, plague, smallpox and different fevers that killed most people during the crises. As an example, in the middle of the 18th century 50% of all deaths in the age group 1-5 years in Sweden were due to smallpox. Furthermore, fevers and dysentery during the supply crises in the 1740s and 1770s were horrible with tens of thousands dead. As a result, many studies have attempted to capture the significance of the epidemics; how long have they been around, how high mortality did they caused, how were they perceived and how have the attempts to prevent their spread looked like. This means we have a fairly good understanding about which diseases have caused misery for people around the world.
When it comes to the important questions regarding where the epidemics originated, what distribution they had and, above all, how they spread, we know very little. The material historians can use for this are statistics from the time, reports and church books. Disease historians have tended to focus on the mid/late 18th century – a time for which “ready” statistics were starting to appear and diagnoses and source material are generally better. However, by then “The age of pestilence and famine” for the Europeans” was since long over. The diagnoses made and the information in the 18th century church books and doctor reports are not as sure: there are dialectal terms for diseases and the different understanding about their cause and their way of spreading meant that the reasoning with regards to illness was different. Another central problem is that in the few studies that have been conducted the study areas have generally been limited to a local community or separate country whereas to our research group it is apparent that diseases were seldom restricted to administrative borders. If we are to understand the historical epidemics, comparative analysis need to be made for independent outbreaks in different countries’ port cities and market places in various regions with no regards for administrative units.
Though a collaboration between researchers from Sweden and Estonia and GIS expertise from the Center for Digital Humanities the goal with the project is to explain the spread of a few of the worst 18th century diseases in area of the Baltic Sea; dysentery, smallpox and fevers. The research team competence includes demography, GIS, disease history, crisis history and the team has large empirical experience. Our study area is continuous but greatly varying which means analytical advantages. It includes Sweden and Norway separated by a long border, Sweden and Finland with their common political history, the important port city Tallinn and the trade across the Baltic Sea – areas that seldom has been connected in disease historical context.
Some of the big epidemics are closely tied to the individual’s nutritional station, some thrived inside among humans in the winter time, while other spread via water, mostly in the late summer, or hit a certain age group especially hard. Climate, topography, social contact, differences in how life looked, and differences in measures taken to prevent disease spread mattered for the character of the epidemic and its spread. We know that the epidemics have killed several million people, affected societal development and wars – but the systematic analyses of how they really spread are few.
|
1. Deaths in dysentery in Lima and Transtrand parishes summer 1773.
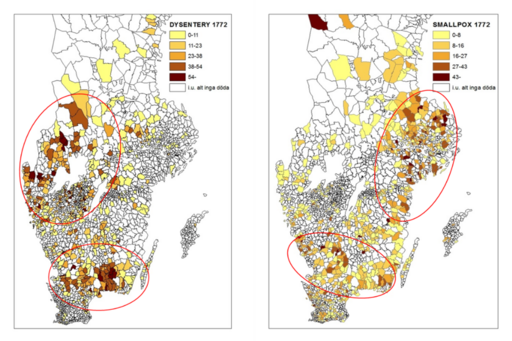
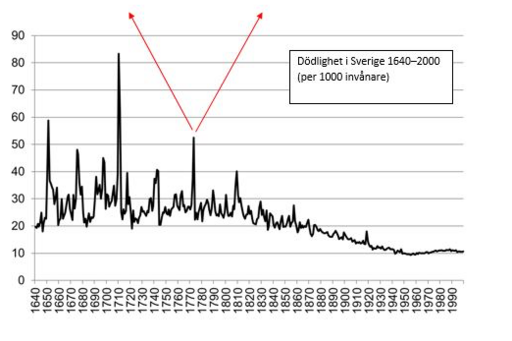
2. Dysentery and smallpox, the famine year 1772 Image
Image
Image
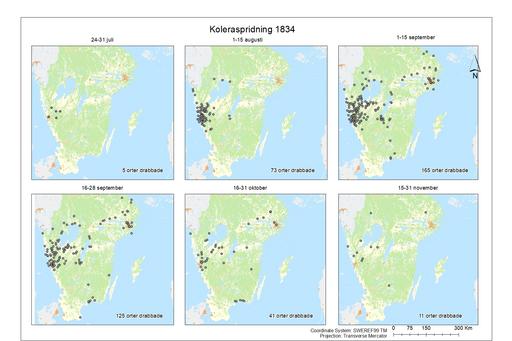
3. Ongoing cholera epidemic 1834 Image
Image

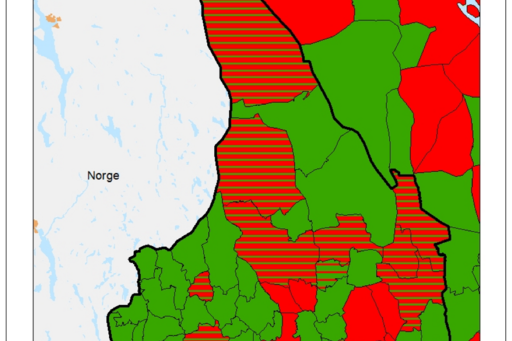
The three groups of illustrations illustrate the limitations and tradeoffs in conducting this type of research – but overall shows nice possibilities of taking this type of analysis further. The animation (1) is one of the results from a pilote study at the individual deaths level of a dysentery epidemic in Lima and Transtrand, parishes in the north western part of the parish Dalarna, 1773. The deaths are tracked day by day. It seems like the epidemic came from the south along the water course Västerdalälven but it is hard to detect any patterns. It is likely related to the time lag between incubation and death during which the infected person may travel far. This potential distance is relatively too big at the parish level and call for bigger study areas. The experiences gained from this pilot means that we have a working methodology and know what types of visualizations can be generated from the final material. We expect to generate a lot more of this type of data during the course of the project. The next example (2) is focused on the famine year 1772. The graph shows mortality in Sweden (Lennart Palm Livet, kärleken och döden. Fyra uppsatser om svensk befolkningsutveckling 1300-1850, Göteborg 2001), and maps based on the data in Tabellverket on parish level. The maps show how smallpox and dysentery were central to the peaks in mortality and also in what parishes the disease was present. The possibility of conclusions with regards to regional centers are hence good. However, there are big gaps in the material which is indicated by a check of the material for Värmland 1773. In Tabellverket’s data dysentery is registered for 58/78 (74%) counties in the Sweden. A check in the death- and burial records of the 20 counties supposedly free from dysentery indicated that there actually was dysentery in 18 out of them. Given this, the actual percentage of counties with dysentery is 97% rather than 74%. The last series of maps show the cholera outbreak 1834, both snapshots of different time periods of the outbreak and the total mortality in cholera for the whole epidemic. The statistics is entirely built on excerption from the death- and burial records. We can see how it spread and observe an interesting center in western Sweden. The purpose of the continued work is to extend the areas and years with individual deaths data. It is not realistic to do it for the whole country, but rather specific regions, epidemics and periods of wars or famines. The gaps in Tabellverket’s data is greater than expected and underline the importance to this work. The empirical and methodological challenges are significant but, at the same time – not least considering the limited knowledge we have about the historical epidemics – with the rich source material and existing digital techniques this project has potential to explain how the epidemics spread. |
Daniel Larsson, Department of Historical Studies
Ida Storm, Centre for Digital Humanities