
Simulations, Models, And RadioTherapy working strategies (SMART II)
Short description
In this project we apply simulations, statistical methods and techniques in a radiotherapy (RT) setting to suggest practical solutions to clinically relevant problems and issues in a whole systems perspective. A first Ph.D. project included mapping of current work practices at Swedish RT departments and system dynamics to test and evaluate different scenarios. Building on previous work, we are continuing our research in this area aiming to improve workflows in RT. The project focuses on efficient data management in RT using real-time data and investigating an automated data-extraction tool for use in external applications, dynamic patient scheduling and medically relevant waiting time. The overall aim is to use a data-driven approach to find strategies supporting RT staff in daily work-related decisions.
Background
Worldwide, increasing number of cancer patients is resulting in a high demand for radiotherapy (RT). Swedish RT is already facing major challenges, especially regarding workload, education, and recruitment of staff.
Considering the current level of resources, the demand can be difficult to meet, and patients may be facing long waiting times. RT is also a time-critical cancer treatment with a radiobiological basis motivating the importance of keeping to a planned schedule not to jeopardize the chances of cure.
To solve operational issues in RT, simulations and computational methods can be a time-efficient way to assist in identifying solutions to areas of improvement. Created models can also predict scenarios about likely effects if results are to be implemented in reality.
To this end, decision support aids in healthcare are designed based on such models and are intended to assist the clinical decision-making process for both healthcare professionals and patients. The concept of decision support can also be applied at a more organizational level to create technical solutions which assist staff in decision-making processes to improve an existing clinical workflow.
Purpose
The overall purpose of this project is to develop and test various decision support strategies to assist RT departments in streamlining their work given existing number of staff and available equipment for treatment delivery.
The hope is that the project will provide increased opportunities for RT managers and staff to optimize the use of limited resources with maintained or improved safety, treatment quality, workload, and patient satisfaction.
Objective
Our goal is to enable the use of stored RT data in Oncology Information Systems (OIS) for various applications in RT using a data-driven approach to find strategies supporting daily work-related decisions at RT departments.
Results
Previous results from the project have been summarized in one PhD thesis from 2021 (1).
Project 1 – Data extraction tool
In the next PhD project, we created a tool for automatic OIS data extraction, cleaning, and formatting since stored information in the OIS is commonly in an unstructured format and needs to be processed before use. The tool was tested using the data from a large RT department in Sweden and successfully created ready-to-use datasets for external use. The time taken by the tool to prepare the datasets was significantly less compared to manual preparation with results close to a manually - prepared reference dataset. We also tested the tool-created dataset as input to an example external application and found that the result using the tool dataset was similar to the result using the reference.
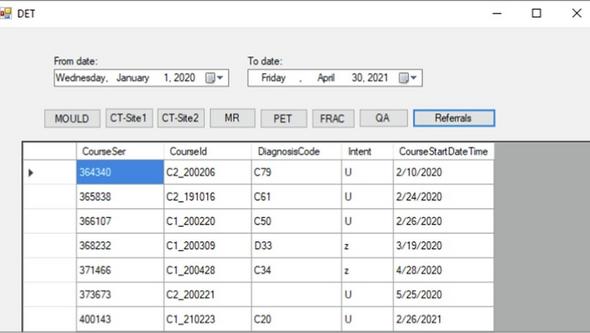
The tool was tested using the data from a large RT department in Sweden and successfully created ready-to-use datasets for external use. The time taken by the tool to prepare the datasets was significantly less compared to manual preparation with results close to a manually-prepared reference dataset. We also tested the tool-created dataset as input to an example external application and found that the result using the tool dataset was similar to the result using the reference.
Project 2: Patient scheduling algorithm
In continuation with the data extraction tool, we further developed and evaluated a sorting algorithm to assist in the scheduling of patients for treatment using real-world scheduling data from the OIS. Our strategy automated the principles of the manual scheduling process and balanced individual patient-treatment characteristics with available treatment slots. In comparison with manual allocations, the algorithm resulted in less expected overall waiting time by changing the distribution between low and high priority patients. The algorithm prioritized patients based on preferred start dates and not solely on clinical priority, allowing more flexibility to schedule patients with tighter deadlines and making the process easier with potentially more available slots to choose from. Quarterly comparisons between diagnosis groups revealed that some patients from the larger diagnosis groups could wait longer while patients from other smaller diagnosis groups could be scheduled earlier. Overall, the algorithm produced quick results and has the potential to make the scheduling task more time efficient for the scheduling staff.
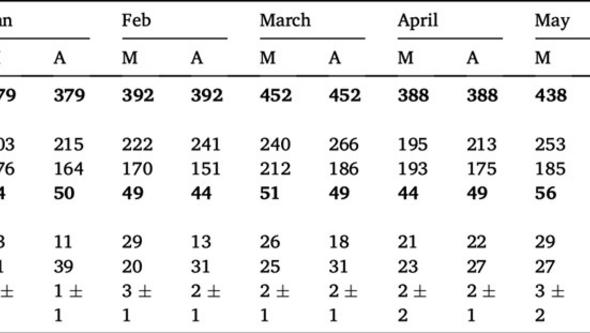
Figure 3: Comparison for manual scheduling and algorithm suggestion for the first the first half of the year 2022 (January to June).
Abbreviations: M- Manual allocation, A- Algorithm output.
Note: High and Low priority is based on the algorithm’s assessment levels and do not necessarily reflect clinical priority levels. Delays were calculated using patient’s referral date, ideal start date and actual start date for both manual and automated calculations.
Project 3: Waiting time comparisons and complexities
The second part of project 3 included comparisons and analysis of different waiting time definitions explored in Project 2. This study highlighted the ambiguities of measuring patient delays and investigated three approaches to depict the waiting time in RT. With access to detailed scheduling data (Year - 2023) from the RT department at Sahlgrenska University Hospital, preliminary results indicate that using the referral dates as the starting point for waiting time calculations resulted in an overall delay distribution that peaked around 4 to 5 weeks past that date. Using prioritized treatment start dates, the peak was 1 to 2 weeks after the soft deadline indicating the earliest point in time when treatment should start. The peak was one week prior the hard deadline indicating the latest point in time when treatment should start. Alongside diagnosis and booking category-specific considerations when assessing delays, analyses of questionnaire responses and a recent public dataset from different-sized RT departments across Sweden showed that there was no consistent waiting time definition used nationally, nor was any single definition more commonly adopted than others. Overall, comparisons suggest focusing on preferred start dates for a better understanding of patient timelines. Referral to RT start as a basis for delay calculations could still be useful for patients with no other procedures before RT.
Ongoing work
Project 4: Qualitative analysis
Ongoing work includes a qualitative analysis where we collect information about workflow changes in RT and investigate how they relate to availability of RT treatments at one of Sweden’s largest RT departments. Senior oncologists, medical physicists and oncology nurses/RTTs working at the Sahlgrenska University Hospital (SU) RT department were contacted in 2023 and asked to participate in a semi-structured interview about their experiences of events in the RT workflow during the last decade including the handling of the pandemic period. All interviews have been summarized, and the content is currently being categorized in themes according to the qualitative analysis approach proposed by Braun and Clarke. Quantitative data on the number of treated patients and fractions delivered during the studied period will supplement the qualitative findings. Preliminary results suggest that there some key factors associated with patient volumes that are captured solely through interviews, such as organizational events or effects of technical changes.
PARTICIPANTS SMART II
Internal:
Mruga Gurjar
Jesper Lindberg
Thomas Björk-Eriksson
Caroline Olsson
External:
Caroline Adestam-Minnhagen
Previous (SMART):
Paul Holmström
Stefan Hallberg.
PUBLICATIONS
(1) Jesper Lindberg: Towards a balanced radiotherapy workflow using practical solutions identified by field studies and simulations, Göteborgs universitet 2021
(2) Mruga Gurjar: Automated data extraction tool (DET) for external applications in radiotherapy, TIpsRO 2022
(3) Mruga Gurjar: Effectiveness of Dynamic Prioritization for patient scheduling: A Discrete-Event Simulation Model, Abstract, ESTRO 2021