
Endometrial Cancer - Studies on recurrences, complications and preoperative diagnostics
On Mars 31, Åsa Åkesson is defending her thesis for Doctor of Philosophy in Medical Science at the Institute of Clinical Sciences, Sahlgrenska Academy, in the research subject of Obstetrics and Gynecology
The title of the thesis is: Endometrial Cancer - Studies on recurrences, complications and preoperative diagnostics
Link directly to the doctoral thesis

ABSTRACT:
Background:
Primary treatment for endometrial cancer (EC) is surgical with hysterectomy and bilateral salpingo-oophorectomy and added lymphadenectomy fo staging.
Aim:
The aim of this thesis was to study recurrence, survival, and surgical complications in a population-based cohort and to assess the introduction of the first national guidelines (NGEC). A second aim was to evaluate preoperative risk classification with transvaginal ultrasound (TVUS) and magnetic resonance imaging (MRI) in low-grade endometrioid EC.
Methods:
In Paper I-III, data from the Swedish Quality Register for Gynecological Cancer was retrieved and completed with medical records reviews. Survival and regression analyses for risk factors were performed.
Paper IV was a prospective multicenter study in the WSHCR including patients with low-grade EC. Myometrial infiltration (MI) and cervical stroma invasion (CSI) were assessed with both TVUS and MRI and the methods were analyzed for diagnostic accuracy and compared.
Results:
The recurrence rate was 8.3% in endometrioid (Paper I) and 29% in non-endometrioid EC (Paper II). The total 5-year DFS was 83.9% and 61.9% for endometrioid and non-endometrioid EC respectively. If no recurrence occurred, the 5-year OS was 91.9% in endometrioid and 88.5% in non-endometrioid EC. The OS increased from 57.3% to 72.0% after the implementation of NGEC (Paper II). SurgicalClavien-Dindo complications grade >II occurred in 19.7% and surgical technique, obesity and lymph node dissection, were found to be independent risk factors (PaperIII). In Paper IV, MRI had a higher accuracy for deep MI than TVUS, but no difference in sensitivity.
Conclusions:
The survival was excellent when no recurrence occurred, in both endometrioid and non-endometrioid EC. A significant improvement in survival was seen in non-endometrioid EC after implementation of NGEC with lymph node staging, despite less adjuvant radiotherapy administered. For the assessment of deep MI, MRI had a higher accuracy than TVUS. The sensitivity of TVUS performed by gynecologists was evaluated as acceptable and did not differ from MRI.
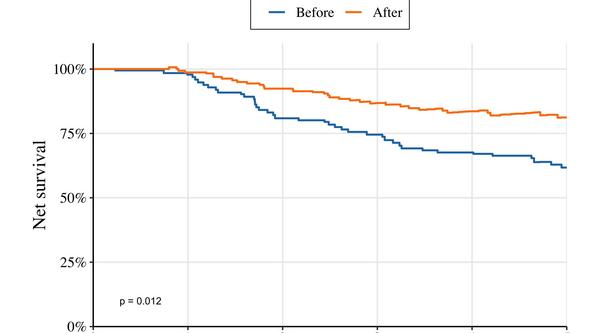
Figure 20B. 5-year NS for non-endometrioid EC before/after NGEC (Paper II)
Supervisor: Pernilla Dahm-Kähler
Co-Supervisors: Henrik Leonhardt and Ian Milsom
Opponent: Frédéric Amant, Katholieke Universiteit/University Leuven, Leuven, Belgium
Examining committee: Andreas Muth, Päivi Kannisto och Johan Stranne