
- Home
- Research
- Find research
- Inflammatory skin diseases, cutaneous lymphomas and genodermatoses
Inflammatory skin diseases, cutaneous lymphomas and genodermatoses
Short description
The research comprises clinical and experimental studies of inflammatory skin diseases, primarily psoriasis, atopic dermatitis and cutaneous lymphomas. Projects investigate vitamin D levels, phototherapy effects, and analyze lipids, vitamin D and its receptors in skin tissue using methods such as mass spectrometry imaging, RNAscope® and immunohistochemistry. Studies also examine circadian regulation of skin biology and its alteration in psoriasis, as well as links between skin disease, depression, the gut microbiome and lifestyle factors. Additional work includes development of evaluation tools, treatment outcomes in atopic dermatitis based on the SwedAD registry, and epidemiological studies of skin disease in Västra Götaland.
Our research projects
Vitamin D is a cholesterol-derived hormone produced in the skin upon exposure to ultraviolet B radiation (UVB) and plays a central role in keratinocyte proliferation and differentiation.
Atopic dermatitis (AD) and psoriasis are the most common inflammatory skin diseases, affecting approximately 10% and 3% of the population, respectively. Cutaneous lymphomas are rare and currently incurable diseases, where approximately one in ten affected individuals develop a severe disease course with spread to lymph nodes and internal organs.
The risk of cutaneous lymphoma is increased in individuals with inflammatory skin disease, but the underlying mechanisms are not yet fully understood.
The health effects of vitamin D are well studied, yet associations between serum vitamin D levels and clinical outcomes have shown inconsistent results. One possible explanation is limitations in how vitamin D status has been assessed, where free vitamin D in serum may be a more relevant biomarker than total vitamin D levels.
Our research group therefore studies vitamin D metabolism in patients with inflammatory skin diseases and cutaneous lymphomas by analyzing blood and skin samples before and after different treatments. In previous studies, we have analyzed free vitamin D and vitamin D-binding protein (DBP) in patients with AD and psoriasis to evaluate their clinical relevance. In a larger patient cohort, we will further analyze vitamin D-related molecules and inflammatory parameters in blood.
Both inflammatory skin diseases and cutaneous lymphomas can be effectively treated with UVB phototherapy. The treatment has well-documented immunomodulatory effects and is thought to be partly mediated via vitamin D. However, it remains unclear whether vitamin D production differs between healthy and diseased skin. Several aspects of vitamin D metabolism in these patient groups are also not yet fully characterized.
Our studies investigate how UVB exposure affects local vitamin D production in the skin, its relationship to serum levels, and its effects on local and systemic inflammation in AD, psoriasis and cutaneous lymphomas. Advanced methods such as RNAscope® in situ hybridization, immunohistochemistry and mass spectrometry imaging are used.
The overall aim is to increase understanding of the role of vitamin D in inflammatory skin diseases and cutaneous lymphomas, thereby enabling more individualized vitamin D treatment for selected patient groups.
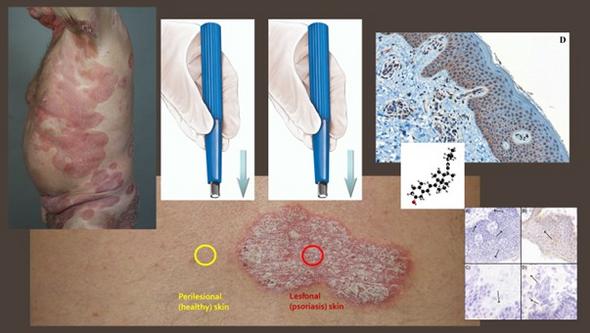
Vitamin D is a hormone produced in the skin upon exposure to ultraviolet B radiation (UVB). In addition to its well-established role in skeletal health, vitamin D also has immunomodulatory effects that may be relevant in both atopic dermatitis (AD) and psoriasis. UVB phototherapy is an effective and established treatment for both conditions. We hypothesize that the therapeutic effect of UVB treatment in the skin may be linked to the local production of vitamin D.
In this research project, we have therefore focused on analyzing the vitamin D receptor (VDR) and vitamin D-binding protein (DBP) in skin tissue. The aim is to map how VDR and DBP are expressed in the skin of individuals with AD and psoriasis, and whether and how this expression is influenced by different treatment methods.
Skin samples have been collected from patients with AD and psoriasis, both from affected skin and from apparently unaffected skin, before and after different treatments. Patients with AD received UVB phototherapy, while patients with psoriasis were treated with either UVB phototherapy or a biological drug (etanercept). The skin tissue has been analyzed using immunohistochemistry and RNAscope® in situ hybridization.
The results from this project are expected to provide a deeper understanding of the role of vitamin D in AD and psoriasis at the molecular level. The knowledge generated may contribute to the development of more individualized treatment strategies. The methods are also planned to be used in future studies of patients with cutaneous lymphomas and other inflammatory skin diseases.
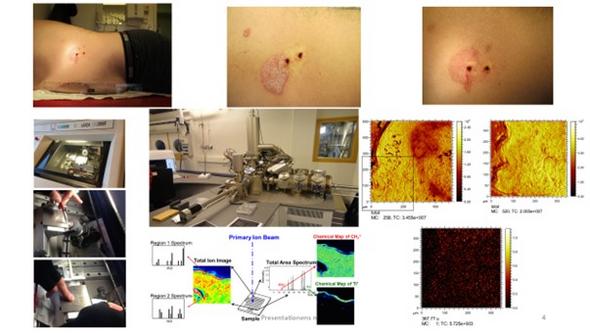
Time-of-flight secondary ion mass spectrometry (TOF-SIMS) is an imaging technique that can identify both elements and organic molecules. In pilot studies, we have demonstrated a novel application of this method that enables the study of the distribution and quantification of lipids, vitamin D and its metabolites in the skin. TOF-SIMS therefore represents a valuable tool in our subprojects.
Metabolic syndrome, including obesity and lipid disturbances, is common among patients with psoriasis. Obesity is associated with more severe disease and may also reduce the response to treatment. Several studies have shown that adipose tissue is involved in the development of psoriasis through systemic effects on the skin. This influence has previously been linked to abdominal fat, but more recent findings indicate that subcutaneous fat may have a direct effect on the overlying skin.
Using advanced microscopy techniques (non-linear microscopy (NLM) and mass spectrometry imaging (MSI)), we have shown that lipid content in psoriasis plaques is higher than in unaffected skin and normalizes following phototherapy. If the lipid profile improves with light and/or systemic treatment, this suggests that early treatment of psoriasis, through its effects on lipid metabolism in the skin, may reduce the risk of comorbidities associated with disturbed lipid metabolism. Further studies using newer techniques are needed to better understand the role of these observed local lipid changes in systemic inflammation.
Our use of MSI, including TOF-SIMS, to study lipids and vitamin D in skin and subcutaneous fat provides unique opportunities to visualize the distribution of these molecules in the biochemical processes of the tissue and to quantify their metabolites.
The main aim of this project is to define how time of day affects biological function in human skin and how this temporal regulation is altered in inflammatory skin diseases. By combining ex vivo models of human skin with multi-omics analyses, the project will generate the first circadian atlas of healthy human skin, capturing dynamic changes in gene expression and proteins over the course of the day.
This atlas will serve as a reference framework for investigating temporal dysregulation in psoriasis and other skin diseases, potentially contributing to a more precise understanding of disease mechanisms and laying the foundation for time-adapted dermatological treatments.
Psoriasis and atopic dermatitis (AD) are inflammatory skin diseases associated with a wide range of symptoms. Psoriasis is an immune-mediated systemic disease that can involve the skin, joints, nervous system and gut. AD, in contrast, is characterized by a defective skin barrier combined with an overactive immune response. The impact of these diseases extends beyond physical symptoms and can have significant consequences for self-esteem and social life, making them important to understand from both medical and psychosocial perspectives. Depression is characterized by persistent low mood and reduced interest or pleasure.
Several previous studies have shown that inflammatory skin diseases and depression have a bidirectional relationship and may influence each other. In both conditions, signs of increased systemic inflammation have been observed. Studies have also shown that both the bacterial and fungal composition of the gut microbiome is altered in patients with psoriasis and depression compared with healthy individuals. The aim of the conducted studies was therefore to investigate how the gut microbiome, including both bacteria and fungi, changes in patients with psoriasis during treatment with biological drugs. At the same time, inflammatory parameters were analyzed, including calprotectin in feces and serum as well as multiple cytokines.
The composition of the gut microbiome was analyzed through sequencing of the V3–V5 region of the 16S rRNA gene for bacteria and the ITS2 region for fungi. Correlation analyses were also performed with several scoring scales and lifestyle factors in order to identify potential associations with specific microorganisms. Calprotectin was analyzed using ELISA, and cytokines using ELLA technology. This is a relatively new and still underexplored research field, and these initial studies provide important descriptive knowledge as a basis for future, more comprehensive investigations.
The studies conducted so far included patients who were initially treated with TNFα inhibitors but later showed insufficient treatment response. These patients were therefore included prior to switching to brodalumab, an IL-17 receptor inhibitor. Fecal and serum samples were collected before the treatment switch and again 12 weeks after initiation of the new treatment. TNFα and IL-17A are pro-inflammatory cytokines that drive immune activation and inflammation, particularly in autoimmune and inflammatory diseases. Inhibition of these cytokines leads to reduced inflammation and tissue damage, which can alleviate disease activity, but may also be associated with a somewhat increased risk of infection.
The analysis showed that the majority of bacteria belonged to the dominant bacterial phyla Firmicutes and Bacteroidetes, while Ascomycota was the dominant fungal group. No significant changes in the composition of the gut microbiome were observed after switching to brodalumab, and no specific bacterial or fungal taxa could be linked to the severity of psoriasis or depression. Calprotectin levels were elevated in patients with psoriasis but were not significantly affected by the treatment switch. An increase in serum IL-17A was observed, which is consistent with the mechanism of action of brodalumab. Because the drug blocks the IL-17 receptor A rather than directly neutralizing IL-17A, receptor-mediated degradation of the cytokine is prevented, leading to accumulation in the circulation without reflecting increased systemic inflammation. No significant changes were observed in the other cytokines analyzed.
The finding that the gut microbiome did not change after treatment is valuable and contributes to a better understanding of how biological drugs affect the body. This knowledge may, in the future, form the basis for more individualized treatment strategies in psoriasis. Similar studies are also planned for other inflammatory skin diseases and cutaneous lymphomas. The goal is to conduct larger and more comprehensive studies that can provide a clearer picture of the role of the gut microbiome in psoriasis, including the incorporation of metagenomic analyses in larger patient cohorts than have previously been studied.
The study is a collaborative project between the Department of Dermatology at Sahlgrenska University Hospital (SU) and rheumatology units within the Västra Götaland Region (VGR), including SU, Skaraborg Hospital (SkaS) in Skövde, and Södra Älvsborg Hospital (SÄS) in Borås.
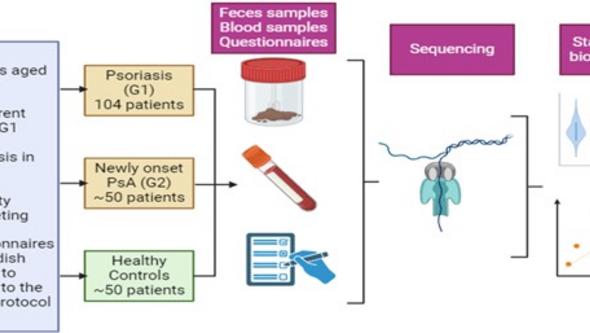
The aim is to follow and compare, in parallel, patients with psoriasis (PsO), newly diagnosed psoriatic arthritis (PsA), and rheumatoid arthritis (RA), in order to identify predictors of disease course and severity, treatment response, comorbidities, quality of life, and health economic outcomes.
Patients with PsO as well as newly diagnosed PsA and RA are included in the study. Research visits are conducted at inclusion and after 1 and 3 years, with planned follow-ups also after 5 and 10 years. At each visit, clinical examinations of the skin and joints are performed, and patients complete structured questionnaires.
Extensive sampling is carried out, including serum, plasma, peripheral blood mononuclear cells (PBMC), DNA, RNA, and feces, for future analyses of biomarkers, genetic factors, autoantibodies, and microbiota. Skin biopsies are obtained from patients with psoriasis. Patient inclusion is currently ongoing intensively at all participating study centers.
The study is expected to serve as a long-term platform for a large number of research projects. The figure below illustrates an initial flow chart, although the final cohort is expected to be larger than indicated.
This study is a collaborative project between Gastroenterology, Dermatology, and Rheumatology at Sahlgrenska University Hospital (SU).
The aim is to individualize, simplify, and improve monitoring of patients with psoriasis (PsO), psoriatic arthritis (PsA), and rheumatoid arthritis (RA) treated with methotrexate (MTX), and to identify predictors of liver fibrosis by combining routine blood-based assessment (FIB-4) with novel fibrosis markers and imaging.
Patients with PsO, PsA, and RA treated with MTX (>3 months – 10 years) are included in the study from the dermatology and rheumatology clinics at SU. Controls consist of patients with the same diagnoses but without MTX treatment.
Data collection includes cumulative MTX dose, previous liver values, components of metabolic syndrome, lifestyle factors (alcohol consumption, smoking, physical activity), comorbidities, medication, and blood sampling.
All patients undergo non-invasive liver assessment using two methods: transient elastography (TE) and acoustic radiation force impulse (ARFI). Results from TE and ARFI are analyzed in relation to the other collected data using statistical analyses.
Aim: to investigate the relationship between psoriasis, comorbidities, and lifestyle factors such as obesity, physical fitness, and stress.
In completed large registry-based studies using data from, among others, the Swedish Military Conscription Register, we have demonstrated a link between low physical fitness at the age of 18 and an increased risk of developing psoriasis later in life (Press release). Using data from the same register, we have also demonstrated a link between low stress resilience at age 18 and an increased risk of developing psoriasis later in life (Press release).
In the ongoing BEST-Pso project, given the strong association between psoriasis and obesity, we are investigating how bariatric surgery affects psoriasis disease activity. BEST-Pso is a prospective long-term follow-up study of patients with psoriasis undergoing obesity surgery, along with a control group.
The study is part of the randomized controlled multicenter study BEST, which compares the outcomes of the two most common bariatric procedures (gastric bypass and sleeve gastrectomy). Patients are followed over five years with questionnaires assessing, among other factors, disease activity, impact on quality of life, and comorbidities such as depression and joint symptoms.
In the ongoing Gen-Pso project, which is part of BEST-Pso, the prevalence of genital symptoms in psoriasis and their impact on sexual function over time are being mapped.
Aim: to develop tools for reliable remote assessment of psoriasis.
To adapt psoriasis assessment to increasingly digital healthcare, we have translated and validated a self-monitoring tool for psoriasis into Swedish (Link to publication). We are now planning to validate the tool on a larger scale.
In collaboration with dermatology departments at other Swedish university hospitals and the patient organization Atopikerna, studies are conducted on the effects and side effects of conventional and new systemic treatments for atopic dermatitis.
The studies are based on real-world data collected through SwedAD (the Swedish national quality register for atopic dermatitis) and other national health registers. The projects aim to identify factors that are important for optimal treatment selection and outcomes.
Topical steroid withdrawal (TSW) is described as a side effect of topical corticosteroid use, primarily characterized by intensely red and painful skin. The proposed mechanism is a dependence on corticosteroids leading to withdrawal symptoms when treatment is discontinued.
TSW is widely discussed online and on social media, largely driven by testimonies from affected individuals. Healthcare providers have taken a cautious approach to TSW as a concept, as there are many possible explanations for the symptoms (related both to corticosteroids and the underlying disease), in addition to a hypothetical dependency mechanism.
In the absence of a clinical definition, we are conducting survey and interview studies in which research participants with atopic dermatitis who identify as having TSW characterize their symptoms and experiences. The aim is to contribute to a clinical description of TSW that can define populations for further studies of possible underlying causes.
The project is a collaboration between Linköping University, Umeå University, and the patient organization Atopikerna, led by Mikael Alsterholm at Sahlgrenska Academy.
TSW research project in the media:
Link to Swedish Radio feature
Mycosis fungoides (MF) and Sézary syndrome (SS) are cutaneous T-cell lymphomas that are chronic conditions and are considered treatable but not curable.
Sézary syndrome is a more aggressive subtype that involves not only the skin but also blood and lymph nodes. Diagnosis of cutaneous lymphoma can be challenging, and both clinical presentation and symptoms vary considerably depending on disease stage.
Despite the severity of the disease, knowledge of epidemiological and clinical characteristics, histopathology, immunophenotypes, and underlying molecular biology remains limited.
Although considered incurable, treatment of cutaneous lymphomas can halt disease progression, reduce pruritus, and achieve disease control. Both local and systemic treatments are used, but it remains unclear which treatment strategies are most effective.
In our retrospective, registry-based study of MF patients in Västra Götaland, the majority were diagnosed at early disease stages and showed good survival. However, time to diagnosis was long, with a median of 3.3 years. Increased risk of cardiovascular disease and a higher risk of secondary malignancies were observed.
Treatment strategies were appropriately adapted to disease stage, highlighting the importance of topical corticosteroids as an integral part of therapy. Phototherapy (UVB and PUVA) represents effective treatment options in early disease, and may also be valuable in advanced disease in combination with acitretin.
In our study of patients with Sézary syndrome (SS) in Västra Götaland, histopathological findings were non-diagnostic in 20% of cases, and only 35% of patients exhibited the classical triad. Patients had a short median survival of 2.1 years, highlighting the aggressive nature of the disease.
Combination therapy with triple treatment consisting of extracorporeal photopheresis (ECP), interferon-α (IFN-α), and retinoids showed the longest time to next treatment (TTNT), at 14.1 months.
In both studies, a high incidence of skin cancer was observed, motivating further research.
Genodermatoses are inherited skin diseases caused by genetic mutations. These conditions may affect the skin, nails, hair, and sometimes other organs. They vary in severity and clinical presentation.
Most genetic skin diseases are rare. According to the European Union, a disease is defined as rare if it affects fewer than 1 in 2,000 individuals. Rare diseases affect approximately 6% of the global population, meaning that an estimated half a million individuals in Sweden live with a rare disease.
Due to their low prevalence, rare diseases represent a global health challenge. Research, awareness, clinical experience, diagnostics, and treatment options are limited. Many of these conditions are severe enough to impair quality of life or even be life-threatening.
We have previously published a study on 73 different genodermatoses in Sweden between 2001–2020, presenting their incidence and prevalence, which has contributed to a better understanding of healthcare needs in this patient group. In total, we identified 13,318 individuals with genodermatoses, which was higher than previously estimated. (Link to publication)
The most common inherited skin disease in both the local and national cohorts was porokeratosis, with a prevalence of 1:4,000, and an increased risk of keratinocyte cancer and melanoma. (Link to publication).
In one of our research projects, we have investigated how new laser microscopy techniques can improve the diagnosis of porokeratosis, a group of genetically determined skin disorders that often require biopsy for confirmation. The aim was to determine whether modern, fully non-invasive methods could replace or complement traditional histopathology.
We evaluated three advanced microscopy techniques:
- RCM (reflectance confocal microscopy) – provides detailed real-time images of the outer layers of the skin and allows visualization of cellular structures without biopsy.
- MPM (multiphoton microscopy) – uses laser light to image deeper skin structures through tissue autofluorescence. (Link to publication).
- FLIM (fluorescence lifetime imaging) – measures the duration of fluorescence signals and provides information on tissue biochemistry, helping distinguish different tissue alterations. (Link to publication)
The aim of these methods is to develop faster, more patient-friendly and accurate diagnostic tools without the need for tissue removal.
Darier disease
Darier disease is an inherited skin disorder caused by a mutation in the ATP2A2 gene. The defect leads to impaired cohesion between skin cells, resulting in small hyperkeratotic lesions, nail changes, and recurrent flare-ups. The disease is lifelong but varies in severity between individuals.
To map Darier disease in Sweden, we used two patient cohorts:
- A local cohort from Sahlgrenska University Hospital (2016–2020), identified through medical record searches-
- A national cohort from the National Patient Register.
By combining these data sources, we were able to estimate prevalence and study the risk of skin cancer, particularly keratinocyte cancer, in patients with Darier disease. (Link to publication)
We also have ongoing research projects investigating mortality and comorbidity in two other groups of inherited skin diseases: epidermolysis bullosa and ichthyoses. The aim is to better understand disease burden over time and identify risk factors that may improve future care and treatment.