
International postdoctoral studies give a boost to your career and scientific independence
"More professional clinicians should do postdoctoral research, preferably abroad – to get new input and inspiration from other research clusters, learn about new techniques and strengthen their scientific independence," says Magdalena Claeson. Her own research is on malignant melanoma and keratoacanthoma, an unusually fast-growing skin tumour.

“This particular speciality with the focus on skin has everything, I think. Here, you meet people of all ages and genders, and there’s a huge variety of diseases. Digital technology, including teledermatology and also the new biological drugs, has improved our scope for both diagnosis and treatment,” Claeson says. A researcher at the Institute of Clinical Sciences, she is also senior physician at the Sahlgrenska University Hospital’s Department of Dermatology.
She feels that she genuinely has the opportunity to improve people's quality of life, while continuing to develop personally in her profession.
“After finishing my thesis in 2017, which was about the incidence of malignant melanoma in the Västra Götaland region, I wanted to gain international experience and do my postdoctoral research training abroad. So in 2018 I took a leave of absence and went off to Australia for a three-year postdoctoral fellowship in skin cancer epidemiology at the Queensland Institute of Medical Research (QIMR) Berghofer i Brisbane" (1).

This gave Claeson the chance to study thin melanoma and also keratoacanthomas, the latter being a variant of squamous cell carcinoma that can grow very rapidly in the skin within a couple of weeks. Australia is the ultimate part of the world to study both these kinds of tumour, since they are highly prevalent, and because the research is world-class.
Start early with postdoc plans – getting them right may take years
“More clinicians should take up postdoctoral positions, preferably abroad, to get new input and inspiration from other research clusters, learn about new techniques and stand on their own feet scientifically. That way, you can develop independence from your doctoral supervisors, but still get superb guidance from an experienced senior researcher in the postdoc group. For me, the years in Australia also improved my skills in writing project plans, working independently using statistics and supervising students. The postdoctoral period not only helped me to achieve greater scientific independence, but gave me more knowledge about myself as a person and an immensely broader network. My family, who came with me, had an unforgettable time as well.”
But obtaining a postdoctoral position outside Sweden proved to be no simple, straightforward matter. At the University of Gothenburg, there was no well-trodden path for those who wanted to do a postdoc abroad.

“Anyway, I found no specific unit to address all my questions to – the ones that arose about employment conditions, health insurance, leave of absence, rules on using the research grants I’d received, not to mention housing, schools for my children, visa issues, vaccinations and so on. But I had superiors at both the Hospital and the University who knew the importance of research abroad and thought it was a good idea for me to go – and then come back!”
The University should be better at supporting its PhD researchers outside Sweden, she thinks. There is no coherent unit in charge, to give support and guidance. There are numerous practical details that need to fall into place before one can venture to take the step, and for the stay abroad to be practicable for an accompanying life partner and/or children, if any. Claeson also wants to highlight, in particular, the social community aspects, which are more important than people think while they are away.
“Then, when you get back, the University and the Hospital can benefit from your newly acquired skills, experience and contact network. A ‘knowledge centre’ is absolutely essential for this very purpose, to promote internationalisation at Sahlgrenska Academy. As I see it, this is bound to be a win-win situation.”
What is more, it all takes time when you want to explore opportunities of applying for various research grants and decide where in the world you want to go, the scope for taking the family with them and so forth. All this is usually done, too, at the same time as the prospective postdoc is engaged in clinical work, perhaps finishing the doctoral thesis and starting a family. For Magdalena, it took over two years from start to finish – not an uncommon time frame.

“My plan was to take the opportunity provided by a conference in Australia to arrange meetings with selected professors and supervisors. Then I talked to other researchers who knew those supervisors, but whose position wasn’t dependent on them. This whole approach was intended to find the best possible mentor and a research environment that had expertise and would be rewarding and congenial. And lots of people pointed me to QIMR Berghofer and Professor David Whiteman of the Population Health team.(2)
When she met Whiteman, she was given a warm welcome and four different projects to choose from. She chose a collaborative one, involving QIMR Berghofer and the University of Queensland, that was designed to identify prognostic markers for thin melanomas. This project then formed the basis of her grant applications.
Worth making your research-funding application excellent
For anyone wanting to learn how to write a successful grant proposal, Magdalena recommends taking a course. Having an interesting research idea is not enough: you also need to be able to describe the idea in simple terms to the people who are going to read your application. The University’s course “Grant writing”, which she attended in 2016, has proved to be the most useful one she has done to date. Similar courses and workshops are currently available through the Academy’s Research and Innovation Services,(3) which also read and provided assistance with her applications.
“I then opted to get in touch with various research funders to ask what their approval rate was, so that I could make smart choices and spend the bulk of my time on the applications affording the greatest chances of success. I was awarded grants by the Swedish Society for Medical Research (SSMF), the Gothenburg Society of Medicine, the Swedish Medical Society, the Swedish Skin Foundation and the Sahlgrenska University Hospital Funds. Getting all this funding was a basic precondition for me to get started at all.4 But of course, there are several other good ways to plan and implement your postdoctoral research.”
A postdoctoral position can either be funded by a research group who advertise for a postdoctoral researcher or chosen by the applicant personally, who is then engaged on a self-employed basis after obtaining a grant, award or fellowship. To do clinical work with patients in a hospital at the same time, you need to arrange that kind of employment as well, although Claeson herself opted out of this.
Australia a Mecca for skin-cancer researchers
Some 400,000 people in Australia undergo surgery annually for skin cancer. Of these patients, 15,000 are diagnosed with a malignant melanoma and there are 1,700 deaths from the disease every year.5 In Sweden, 4,307 people had malignant melanoma of the skin, and 538 died, in 2020. But the high UV index and many hours of sun exposure are not the only causes of skin cancer in the population. Researchers are also looking for other underlying factors.

“There were two research groups that I alternated between, one being QIMR Berghofer in Brisbane where I focused on population health and skin cancer, and made extensive use of registers. The research group included people from all over the world, with highly differentiated experience, which was immensely valuable. Lab analyses in the melanoma project were done at the University of Queensland under Professor Kiarash Khosrotehrani, who was my supervisor there. He heads the Experimental Dermatology group, who are engaged in translational research and biomarkers.” (7).
Thin malignant melanoma on the scalp is the most deadly
Thin melanoma is the most common form of melanoma in Australia. Ninety-five per cent of those who are treated for this type of melanoma survive more than 20 years, which is an excellent survival rate. But paradoxically, since this patient category is so large, deaths from melanoma are most commonly caused by a thin tumour.
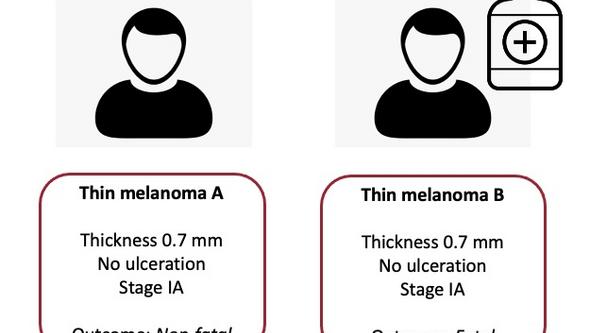
“When thin, thickness ≤ 1 mm, melanomas arise, they spread both in terms of width on the skin surface and of depth. How deep the tumours penetrate into the skin is the important variable, and thickness is closely associated with the outcome. This is why early detection and diagnosis are so important. The question in the postdoc project was: ‘How can we identify, already at diagnosis, the patients with thin melanoma who are not going to survive?”
An ability to identify these particular individuals at the time of diagnosis might make it possible to provide adjuvant (supplementary) treatment and to organise longer follow-up programmes. It would also provide an opportunity for reassurance and less frequent follow-up of people who are at low risk of death.
“We started with a registry study that included more than 27,000 patients with a melanoma measuring up to 1 mm. The data, for the years 1995–2014, came from the Queensland Cancer Register (QCR). Of these patients, some 400 had died and we were able to see that by far the most distinctive risk factor was having the melanoma located on the scalp.”
Why this is so remains incompletely understood, but melanoma on the head entailed six times the risk of dying from the cancer compared with a melanoma of the same thickness that was located elsewhere on the body. Magdalena is now engaged in further work and a forthcoming study of whether identification of prognostic markers through mutational analyses of thin melanomas is feasible.

Keratoacanthoma: a dome-shaped tumour with a central keratinous plug
The other type of tumour Claeson studied, keratoacanthoma, is a very fast-growing, relatively common skin tumour. It is not usually fatal, but may be hard to distinguish from squamous cell carcinoma both with the naked eye and also under a microscope. Keratoacanthoma may be described as a dome-shaped tumour measuring 1–2 cm across, with a central keratinous plug. It may disappear without treatment (undergo spontaneous regression or remission) after several months, but cases of continued growth and metastasis have been described.
“When it came to keratoacanthoma, I had the opportunity to work with a really huge study, a cohort study under way in Queensland with more than 40,000 Australians taking part. It started in 2010 and is the largest prospective skin-cancer study conducted to date worldwide.”
Research data are based on a questionnaire that, initially, all participants were asked to complete. Over the years, these were then merged with laboratory results from various health care units and databases if or when any participant developed skin cancer. Genetic data were then collected from samples of the subjects’ saliva. Subsequent screening revealed 596 participants with keratoacanthoma specifically.
“What we looked at were risk factors, since these haven’t been documented very much, although this tumour type has been known for over a century. What we found was that it’s more common in men and older people with fair skin and freckles; in those who don’t tan easily in the sun, and those who were sunburnt in childhood; and in people who had previously had some other kind of skin cancer."
Smoking and alcohol boost keratoacanthoma risk
The results were not surprising, but the increase in risk caused by smoking and alcohol(8) – a fact picked up by the Australian media – was new (9),(10) For alcohol, the risk was elevated by consumption of more than 14 standard drinks per week, an established national threshold for unhealthy drinking. For tobacco consumption, the risk was higher for research subjects who were active smokers.
In future studies, Claeson will now investigate why this type of tumour can actually regress and disappear without treatment.
“Obviously, we surgically remove keratoacanthomas, because they’re so hard to distinguish from squamous cell carcinoma, which can metastasise. But it sometimes happens that by the time a patient presents for the surgery, the tumour has regressed and disappeared. We’ve started thinking about whether this is due to some kind of immune response in the patient that arises. That’s going to be the focus of my further research, which I’ll be doing partly with the research team in Australia."

So how did all that work and preparation pan out?
Recently, Claeson was appointed to a half-time position under the regional ALF agreement (between Region Västra Götaland and the Swedish state, on cooperation in medical training, clinical research and health care development). This makes it easier for her to concentrate on her research henceforward. The projects included in her ALF application fit into the collaboration she was able to set up thanks to her postdoctoral project in Australia, and she is now leading the projects from Gothenburg. Although her postdoc years were challenging in many ways, and very often arduous and tough, they also gave her an important international view of the research community and good fluency in English –– significant boons.
“I still have my affiliation to QIMR Berghofer. My computer’s still at the office there and by a secure login I can still access the research data and smoothly get on with the job. It’s that simple!”
Text: Susanne Lj Westergren
Sources:
1. Queensland Institute of Medical Research (QIMR) Berghofer, Brisbane
2. David Whiteman of the Department of Population Health, QIMR Berghofer.
3. Research support from the Grants and Innovation Office (FIK), University of Gothenburg.
4. In Swedish: Postdoctoral Grant from the Swedish Society for Medical Research (SSMF), the Gothenburg Society of Medicine (GLS), the Swedish Medical Society, the Swedish Skin Foundation (HudFonden) and the Sahlgrenska University Hospital Funds.
5. QSkin Sun and Health Study, the largest prospective skin-cancer study in the world.
6. In Swedish: the Swedish Cancer Fund’s statistics on the number of people in Sweden found to have malignant melanoma in 2020.
7. Khosrotehrani Group - Experimental dermatology, University of Queensland
8. Study finds ways to reduce the risk of common Queensland skin tumour
9. Queenslanders can reduce skin tumour risk by drinking less and giving up smoking, study finds
10. Radio interview on ABC (Australian Broadcasting Corporation) Radio National show Health Report, with Dr Norman Swan. Australian researchers have published the findings from the world's first large, reliable study of a common skin tumour which is poorly recognised but can be scary. Från 2020, 6:12 minuter.
More about the University’s range of courses
Courses and workshops at the University of Gothenburg on, for example, writing research grant proposals.
More about:
Magdalena Claeson, ResearchGate and her thesis Epidemiology of cutaneous malignant melanoma in Western Sweden.