
Sofie Örnö Ax: Postoperative morbidity in children born with esophageal atresia (EA)
Sofie Örnö Ax's thesis highlights feeding difficulties and health-related quality of life in children born with esophageal atresia (EA). EA is a rare congenital malformation in which the esophagus is not connected to the stomach. Now the results show that these children have many eating and mealtime problems and that the more severe form of EA did not result in worse quality of life than the more common form.

SOFIE ÖRNÖ AX
Dissertation defense: 9 April 2026 (click for details)
Doctoral thesis: Childhood outcomes after esophageal atresia repair
Research area: Pediatrics
Sahlgrenska Academy, The Institute of Clinical Sciences
Esophageal atresia (EA) is a rare congenital malformation in which the esophagus is not continuous, and in most cases the lower part of the esophagus instead connects the stomach to the trachea. In Sweden, 30–35 children are affected each year. These children need surgery as newborns to close the connection to the airways and restore the continuity of the esophagus.
"Survival rates are very good today, over 90 percent, and now that most children survive, we can focus on what they need in order to feel as well as possible while growing up, says Sofie Örnö Ax, surgeon at the colorectal section at Sahlgrenska University Hospital/Östra and a doctoral student at the Institute of Clinical Sciences."
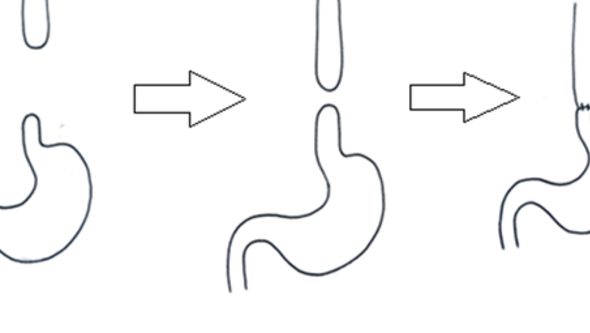
Illustration from thesis with stomach and esophagus: A delayed primary anastomosis means that the gap between the esophageal ends is too long to close during the first operation, when the child is only a few days old. The child is then given a gastrostomy to receive nutrition through, and then you wait 2–3 months, and if the esophageal ends have grown, you can operate again and connect the ends then.

Feeding difficulties are a major problem
The research results show that feeding and mealtime difficulties are common among children with esophageal atresia, and that these problems are also associated with lower health-related quality of life. Parents of younger children report more mealtime difficulties compared with reports from parents of older children.
The more severe form of the condition, which affects about 10 percent of children, means that the gap between the ends of the esophagus cannot be closed during the first surgery. These children receive a gastrostomy and after two to three months doctors attempt to reconnect the esophagus.
"If the gap is still too large, in our patient group it was bridged using either the stomach or the colon. Having the more severe form did not lead to poorer health-related quality of life than the most common form of esophageal atresia, but the children with the more severe form had to undergo more treatments."
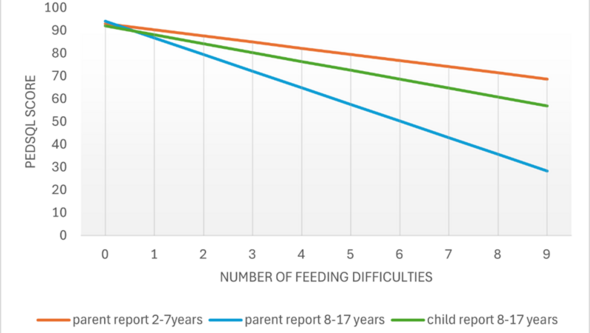
Diagram from thesis: Regression analysis of the bearing of nine feeding difficulties on PedsQLTM4.0 score among children with esophaegal atresia.
Better measurement instruments for patient-reported symptoms during meals need to be developed
"My results show that feeding difficulties are a major problem, despite the fact that I used unvalidated questionnaires, which almost certainly do not capture all the problems these children experience. During the studies, it became clear that we need instruments (questionnaires) that have been developed together with the children themselves and their parents. Without their involvement we cannot know what kinds of difficulties the children truly experience or how we can best help them."
The finding that children with the severe form and the “common” form of the condition have comparable quality of life confirms earlier studies. In practice, this means that clinicians can give hopeful messages early on to new parents going through one of the most difficult situations imaginable – the first period with a newborn baby who is seriously ill.
What has been the most rewarding and the most challenging part of the doctoral project?
"The most challenging part has been that the patient group is extremely small, which makes it difficult to perform robust statistical analyses. It has also been difficult to distinguish between what is “healthy” and what is “ill.” Is it a sign of disease if it takes longer to eat than for one’s friends? If the children themselves do not see it as illness, then perhaps it is not illness, she says, and continues;
What has given me the most is learning a great deal about patient-reported outcome measures and health-related quality of life – how they are measured, why we should measure them, and what it means to see patient encounters and health from the patient’s perspective. It has required some self-reflection and has partly led me to reconsider my own role as a surgeon – a process that I think all colleagues should go through."
Text: Susanne Lj Westergren